ACL graft choices: what are the options?
Choosing the right graft for your ACL reconstruction is one of the most consequential decisions in the surgery planning process. Here's what you need to know about each option.
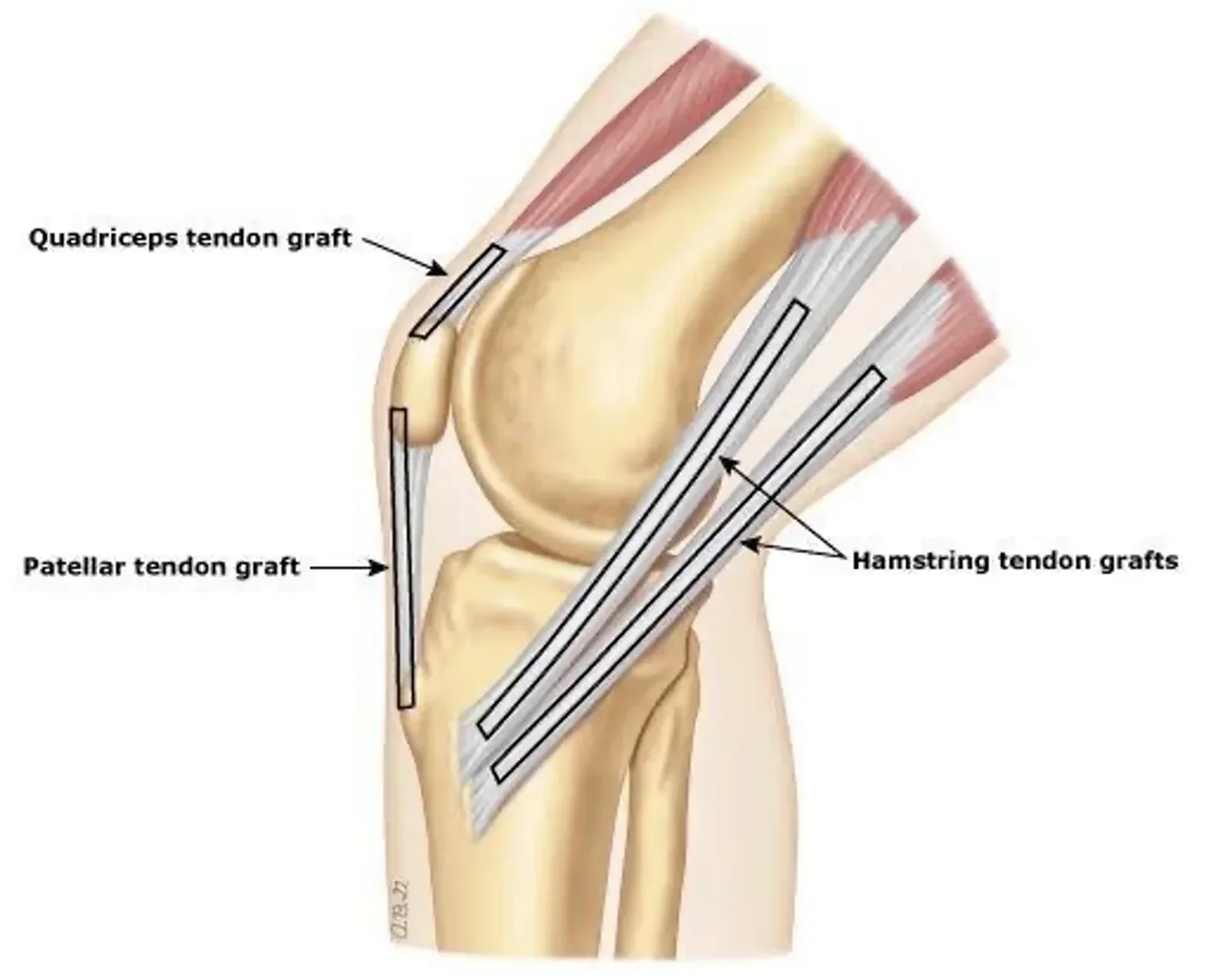
When the anterior cruciate ligament (ACL) tears, reconstruction typically requires replacing the damaged tissue with a graft — either taken from your own body (autograft), from a donor (allograft), or from synthetic materials. Each approach comes with distinct trade-offs in recovery time, re-tear risk, donor site morbidity, and suitability for different patient profiles. No single graft is universally superior; the right choice depends on the patient’s activity level, nature of sport, tolerance of graft morbidity, concomitant injuries and previous surgery.
Bone–patellar tendon–bone (BPTB)
Autograft — middle third of the patellar tendon with bone plugs
PROS
Bone-to-bone healing — theoretically stronger and rapid graft healing
Lowest re-rupture rates in high-demand athletes
Long-term outcome data spanning 20+ years
Reliable graft size and tensile strength
Stiffest graft
Preserve hamstring strength
CONS
Anterior knee pain — especially kneeling
Risk of patellar tendon rupture/tendonitis or patellar fracture
Quadriceps strength deficit in early recovery
Occasional significant knee extension loss
Best for: Young, high-level athletes in pivoting sports (rugby/American football) where re-tear risk must be minimized and in-line running speed needs to be maintained. Revision ACL reconstructions.
Not ideal: Lower demand patients who frequently kneel. Sports that require recurrent jumping or kicking.
Hamstring tendon
Autograft — semitendinosus and gracilis tendons
PROS
Less anterior knee pain than BPTB
Smaller incision and faster early recovery
Good outcomes across a wide patient population
Less damage to the extensor mechanism of the knee
High tensile strength
PROS
Slightly higher re-tear rate versus BPTB in some studies
Tendon-to-bone healing slower than bone-to-bone theoretically
Hamstring weakness in early recovery — relevant for sprinters
Graft diameter can be small in patients with thin tendons
Graft is move elastic and can heal in a more lax state than other grafts
Slight increase risk of infection
Revision for failed graft are more likely to require a 2 stage procedure
Best for: Active adults, recreational athletes, and those wanting to minimise donor site pain and return to light activity levels.
Not ideal: High demand athletes that require straight line running. Patients with lax ligaments (loose jointed) and small sized hamstrings.
Quadriceps tendon
Autograft — central third of the quadriceps tendon, with or without bone plug
PROS
Larger, thicker graft — good for patients needing bigger diameter
Less anterior knee pain than patellar tendon
Can include bone plug for hybrid fixation
Preserve hamstring strength
Stiffer graft than hamstrings
CONS
Donor site discomfort above the kneecap
Less long-term data compared to BPTB and hamstring
Temporary quadriceps weakness and extensor lag possible
The graft can be short and difficult to obtain adequate fixation
Best for: Revision ACL surgery. Young athletes who need to maintain running speed and avoid anterior knee pain morbidity.
Not ideal: Previously failed BPTB graft. Patients with a short quadriceps tendon.
Allograft (donor tissue)
Cadaveric — patellar tendon, Achilles, or tibialis anterior from a tissue bank
PROS
No donor site morbidity — no second surgical site
Shorter operative time and faster early recovery
Useful when multiple ligaments need reconstruction
Good outcomes in lower-demand or older patients
CONS
Higher re-tear rate in patients under 25 returning to sport
Slower biological incorporation of donor tissue
Small risk of disease transmission (very low with modern processing)
Graft processing may reduce structural properties
Best for: Older patients (>35), lower-demand athletes, revision surgeries, and multi-ligament reconstructions where sparing donor sites is critical.
Not ideal: Young athletes who wish to return to competitive sport.
Synthetic ligament (LARS / InternalBrace)
Synthetic — polyester scaffold or augmentation device
PROS
No donor site morbidity
Faster return to sport when used as augmentation
No risk of disease transmission
CONS
Risk of synovitis and particle wear debris
Very high rate of graft failure
Failures require 2 stage revisions
Not recommended as a graft option
Not ideal: Given the high failure rate and forgein body induced synovitis, this graft option should not be offered for the vast majority of ACL injuries.