
Femoroacetabular Impingement (FAI)
Explanation of Diagnosis
FAI, also known as hip impingement, occurs when excess bone in the hip joint causes pinching of the soft tissues during hip flexion. This repetitive contact can lead to damage of the hip labrum and cartilage, resulting in pain and reduced function.
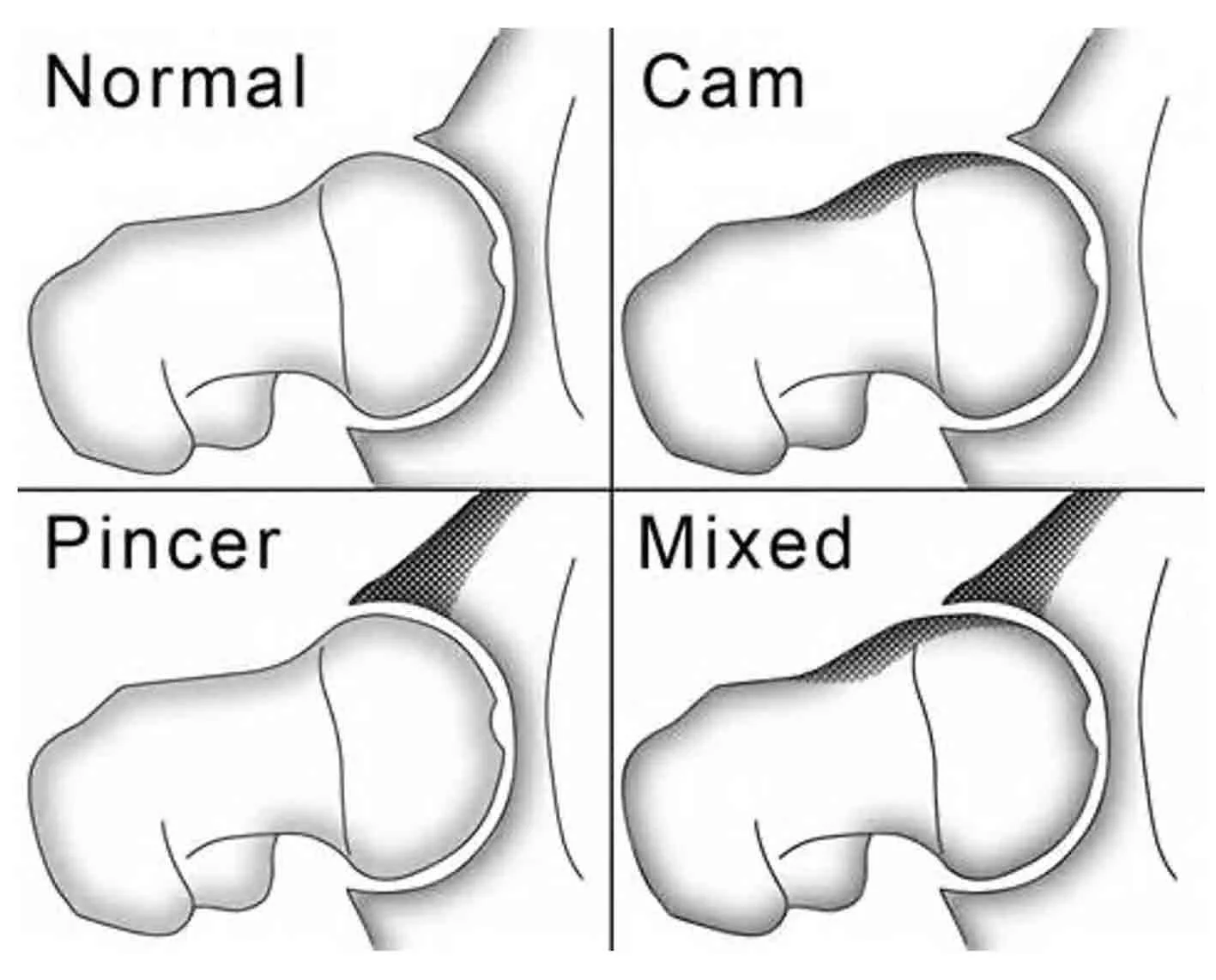
Hip impingement can be classified into three types:
Pincer-type impingement – caused by excessive bone formation along the rim of the hip socket (acetabulum).
CAM-type impingement – caused by extra bone at the junction of the femoral head and neck. Approximately 70% of patients with hip impingement have the CAM type.
Mixed-type impingement – a combination of both CAM and Pincer features.
How did I get FAI?
The shape of the hip socket is largely formed during childhood, while the shape of the femoral head and neck develops during puberty. Recent research suggests that physical activity and sports participation during adolescence influence the development of hip impingement. Studies show that individuals who participate in high-impact or pivoting sports have more than a 90% prevalence of CAM morphology at the femoral head–neck junction.
How is FAI diagnosed?
Diagnosis begins with a comprehensive history and physical examination. Patients with FAI typically report deep groin pain that may radiate to the lateral hip or lower back. Pain is often aggravated by squatting or prolonged sitting. Hip impingement rarely causes “electric” or radiating pain down the leg.
If FAI is suspected, specific X-rays are obtained to assess for abnormal bone formation. Your surgeon may also order advanced imaging such as MRI or CT scans to evaluate hip anatomy in more detail. MRI is particularly useful for assessing labral tears and cartilage health.
A diagnostic injection into the hip joint using local anaesthetic (numbing medicine) is often the final step. Because several other conditions can cause hip pain, temporary relief following the injection helps confirm that the hip joint is the true source of pain.
What is the long-term prognosis?
Patients with CAM-dominant hip impingement are believed to have a higher risk of developing hip arthritis compared to the general population. The repetitive damage to the labrum and cartilage may lead to degenerative joint changes over time. However, more research is needed to determine whether surgical treatment of FAI prevents the later development of arthritis.
Patients with Pincer-dominate hip impingement do not display a higher risk of developing hip arthritis when reviewing current literature.
What if I already have Hip Arthritis?
Patients with advanced arthritis generally do not benefit from hip arthroscopy. Studies show that outcomes are poor in this group, with a high likelihood of needing hip replacement surgery in the following years. Therefore, if you have significant arthritis, a total hip replacement is often the best surgical option for lasting pain relief.
Other causes of Hip Pain
Pain around the hip can arise from several sources. Conditions affecting the lumbar spine (such as nerve compression) may present as hip pain. Likewise, disorders involving other pelvic structures or the surrounding muscles—such as the hip flexors, abductors, adductors, or iliotibial band—can also mimic hip joint pain.
Nonsurgical Treatment
Initial treatment for symptomatic FAI focuses on conservative management, including activity modification, physical therapy, anti-inflammatory medications, and weight loss if appropriate. Physiotherapy can be highly effective in strengthening the hip and core muscles, often reducing or eliminating symptoms.
It is important to understand that not all labral tears require surgery—many people have labral tears without pain. Corticosteroid or biologic injections may also help relieve symptoms. If pain persists despite conservative measures, hip arthroscopy may be recommended.
Surgical Treatment
Hip arthroscopy is a minimally invasive procedure that allows surgeons to repair labral tears and remove excess bone contributing to impingement. The surgery is performed through two or three small incisions in the thigh. Special instruments are used to reshape the bone and restore normal hip mechanics.
During the same procedure, labral tears can be repaired with sutures or reconstructed using a graft if necessary. Damaged cartilage can be smoothed or debrided, although current techniques cannot regenerate new cartilage.