
Robotic Unicompartmental Knee Replacement (UKR)
How is a UKR Performed?
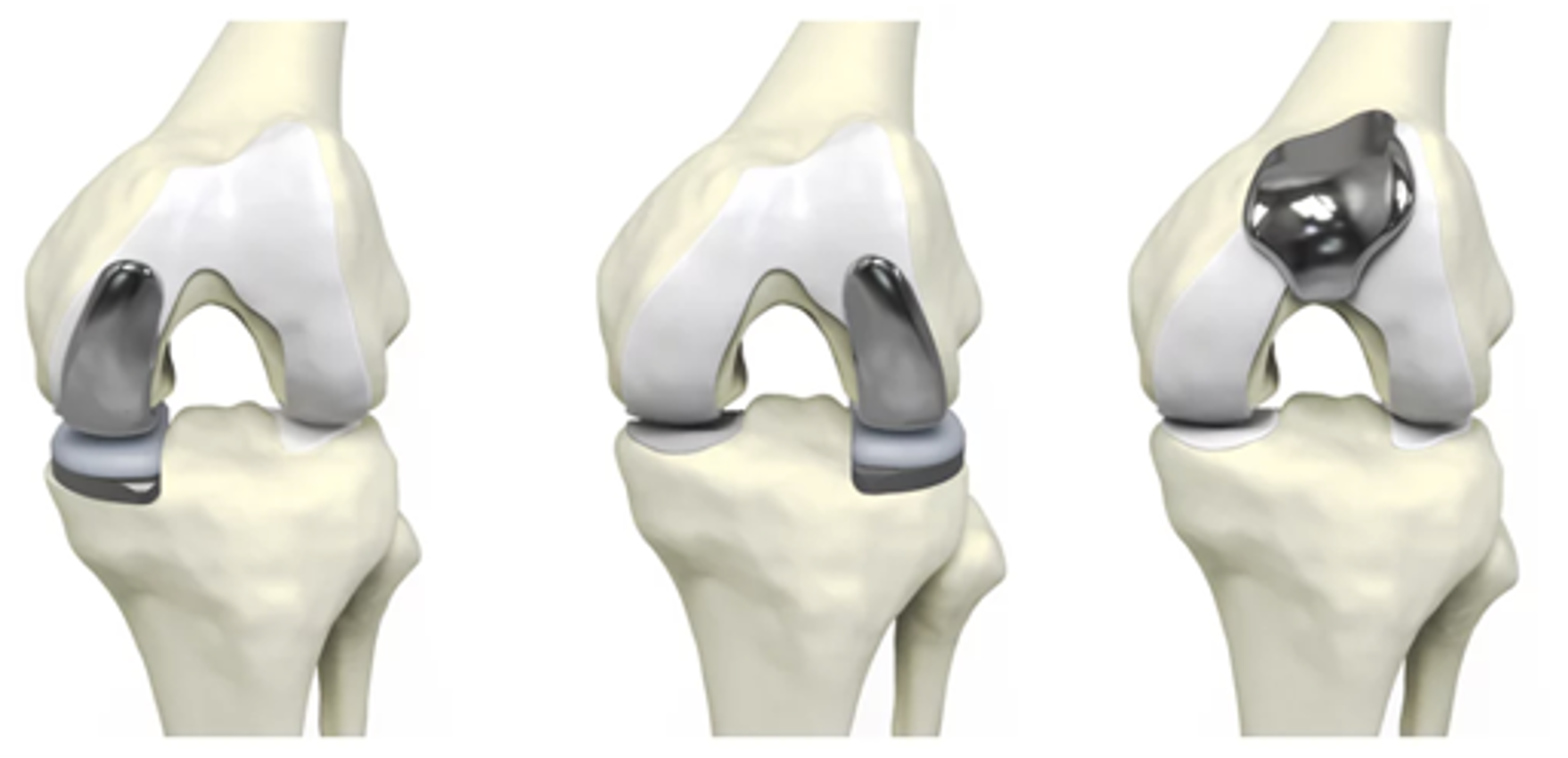
A unicompartmental knee replacement (UKR) — also called a partial knee replacement — is performed when only one part of the knee joint (inner, outer, or patellofemoral compartment) is affected by arthritis, and the rest of the joint remains healthy.
During surgery:
A small incision is made over the knee.
The worn-out cartilage and a small amount of bone are removed from the affected compartment only.
The healthy cartilage and ligaments in the remaining compartments are preserved.
Metal and polyethylene (plastic) components are inserted to resurface the damaged area, restoring smooth joint motion. The metal components are typically cemented in place, but some implants can be fixed in a cementless technique.
The implants are aligned precisely to match your natural anatomy and balance your knee.
Because only part of the knee is replaced, less bone and soft tissue are removed, leading to faster recovery, less pain, and more natural knee movement compared to a total knee replacement.
How Does a Robot Help with Performing a UKR?
Robotic-assisted knee replacement uses advanced computer navigation and a robotic arm to enhance surgical accuracy.
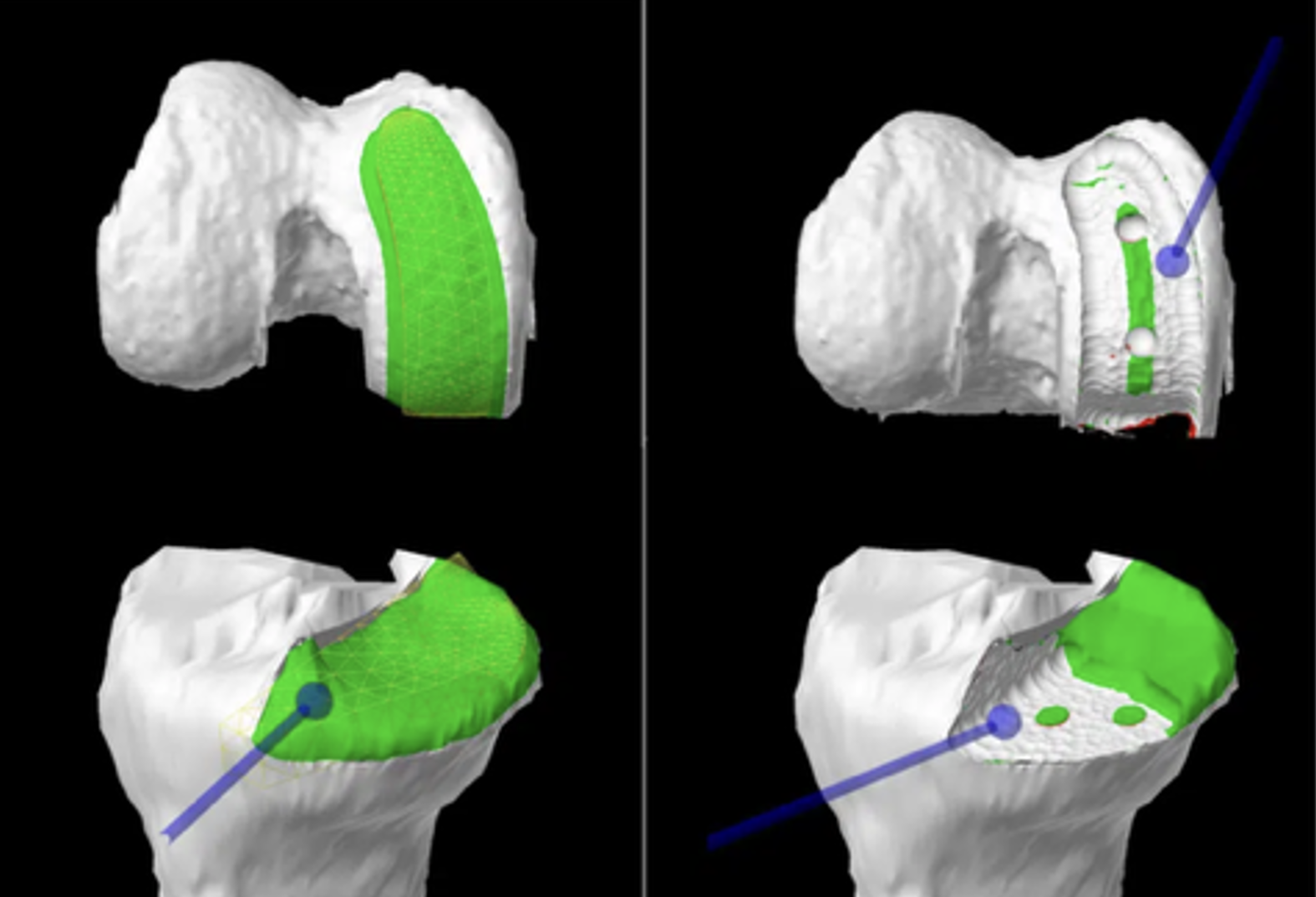
Preoperative Planning: A CT scan or X-ray of your knee is used to plan implant size, positioning, and alignment before surgery.
Intraoperative Guidance: During surgery, the robotic system helps the surgeon perform real-time mapping of your knee and guides instrument placement with a high level of accuracy.
Precision Bone Resection: Certain robots assist with cutting the bone and preserving surrounding soft tissues.
Personalized Fit: Robotic guidance ensures optimal implant alignment and ligament balance, which can improve function, stability, and implant longevity.
It is important to note that the robot is simply a tool that helps your surgeon execute their desired operative plan.
What Is the Recovery in the Immediate Postoperative Period?
Hospital stay: Most patients stay 3 days in hospital working with physiotherapy.
Weight bearing: You will walk on the operated leg immediately with gait aids.
Brace: No braces are required after surgery.
Range of motion: Early motion starts right away.
Ice and elevation: Used frequently to control pain and swelling. You should ice for 20 minutes, 3–4 times per day right after surgery. An ice/compression machine can be hired from a third party.
Assistive devices: You may use a walker or crutches for 2–4 weeks after surgery, progressing to a cane as comfort improves. It can take up to 6-8 weeks before you can walk independently.
How Is the Wound Managed?
Bulky dressings will be removed 1–2 days after surgery.
A waterproof underlay dressing should be left on for 2 weeks.
Incisions typically heal within 2 weeks.
Showers are permitted while wounds are covered with waterproof dressings during the first 2 weeks.
Do not submerge incisions in water (baths, pools, or ocean) for 6 weeks.
A wound check with your GP, allied health provider, or our clinic is recommended at 2 weeks.
Absorbable sutures are usually used and do not require removal, though small remnants may surface naturally during healing.
How Do I Prevent Blood Clots (DVT/PE)?
Blood clots (deep vein thrombosis or pulmonary embolism) can occur after surgery.
You can reduce the risk by:
Moving your foot and ankle regularly while resting.
Walking early with assistance.
Avoiding long periods of sitting or immobility.
Wearing compression stockings for the first 4–6 weeks.
Using compression devices while in bed in hospital.
You will likely take aspirin for 2–4 weeks to prevent DVT/PE. If you have a history of blood clots or risk factors, a stronger blood thinner may be prescribed.
If you plan any long-distance travel within 6 weeks of surgery, please inform our clinic for preventative medication.
Seek immediate medical attention if you develop calf pain, swelling, chest pain, or shortness of breath.
How Do I Manage My Pain After a Total Knee Replacement?
Your anaesthetist will discuss possible spinal or regional nerve blocks to help control pain immediately after surgery.
Local anaesthetic will be injected into the knee during surgery.
Use ice regularly (20 minutes, 3–4 times per day). An ice machine may be hired from a third party.
Take prescribed pain medication as directed. Opioids may be used short-term but have known side effects (nausea, constipation, dependence). Non-opioid medications are preferred when tolerated.
Use a compression dressing on the knee for 6–12 weeks to manage swelling.
Begin gentle range-of-motion and muscle activation exercises as soon as recommended.
Use walking aids for stability while recovering your gait.
What Issues Should I Call the Clinic Regarding?
You should contact your surgeon or clinic immediately if you notice:
Increasing redness, swelling, or drainage from the wound.
Persistent or worsening pain not controlled by medication.
Fever, chills, or night sweats.
Calf pain or swelling (possible blood clot).
Any acute injury to your operative knee.
Prompt review allows early management of potential complications.
When Can I Return to Normal Activities After UKR?
Return to activities depends on the nature and intensity of the activity.
General guideline:
Walking: Start immediately after surgery.
Stationary cycling: Can start right away and is encouraged. Road cycling can take 4–6 weeks.
Light gym exercise (Pilates, pool work, yoga): 6–8 weeks.
Sport (golf, tennis, skiing): Typically 6–12 weeks, depending on intensity.
After surgery, it is important to know that running and high-impact activities are not recommended, as these can damage the implant and surrounding bone over time.
When Can I Drive?
You can usually drive once you can safely control the vehicle and perform an emergency stop comfortably.
This is typically 8–10 weeks after right knee surgery, and 2–3 weeks for the left knee.
You must not drive while taking strong pain medication (e.g., opioids).
When Can I Return to Work?
Return to work depends on your occupation:
Office or sedentary work: 1–2 weeks (once you can commute safely).
Light manual work: 4–6 weeks.
Heavy manual labour: 3–4 months or longer, depending on recovery.
Should I See a Physiotherapist?
Yes. Physiotherapy is essential for optimal recovery and long-term success after UKR.
Your physiotherapist will:
Guide you through a structured rehabilitation program.
Focus on restoring range of motion, strength, balance, and gait mechanics.
Progress exercises gradually from early mobility to functional activity and low-impact sport.
Most patients continue physiotherapy for 3–6 months to achieve full functional recovery.
What Are the Complications After a UKR?
While robotic partial knee replacement is highly successful, all surgeries carry potential risks:
Infection (rare, <1%)
Blood clots (DVT/PE)
Persistent pain or stiffness
Implant loosening or wear over time
Fracture around the implant
Progression of arthritis in the unreplaced compartments
Residual imbalance or instability
Numbness around the incision area
Injury to the extensor mechanism
Poor positioning of the implant
Following your rehabilitation program and attending follow-up appointments will help minimize these risks and ensure long-term success.