
Posterolateral Corner (PLC) Reconstruction
How Is a PLC Reconstruction Performed?
The posterolateral corner (PLC) of the knee is a complex group of ligaments and tendons that stabilize the outer and back (posterolateral) aspect of the joint. It includes structures such as the lateral collateral ligament (LCL), popliteus tendon, and popliteofibular ligament. Together, these control varus (inward bending) and external rotation movements of the knee.
PLC repairs can be performed in rare situations, but repairs have been shown to perform worse when compared to reconstructions. A PLC reconstruction is performed to restore stability after a severe injury or when the knee remains unstable following trauma or multi-ligament injury.
During surgery:
An incision is made on the outer side of the knee.
The common peroneal nerve is mobilized and protected
Damaged structures are identified and either repaired (if acute) or reconstructed using tendon grafts (if chronic or irreparable).
Common graft choices include hamstring tendons or allografts (donor tissue).
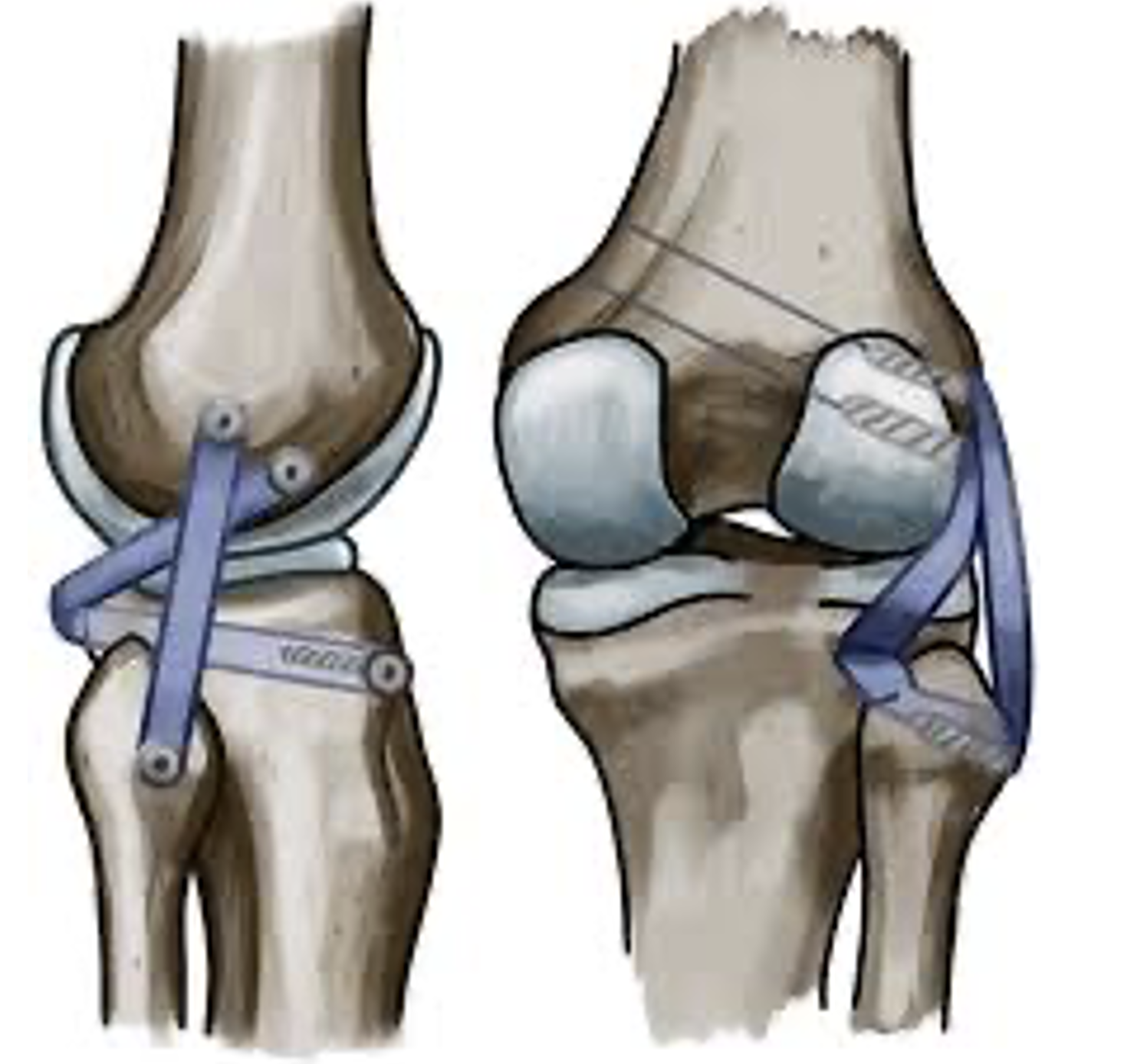
The grafts are placed through tunnels in the femur, fibula, and tibia to recreate the normal anatomy of the LCL, popliteus, and popliteofibular ligaments.
The grafts are fixed with screws or buttons and tensioned in specific knee positions to restore normal alignment and stability.
An isolated PLC surgery typically takes 90–120 minutes, but it is often performed in conjunction with ACL or PCL reconstruction, thus it often takes longer.
What Is the Recovery for PLC Reconstruction in the Immediate Postoperative Period?
Hospital Stay: You will typically only require an overnight stay in hospital. There are situations where discharge home the same day of surgery can occur.
Weight bearing: You will be weight-bearing as tolerated right after with the use of crutches.
Brace: You are typically placed in an unlocked hinged knee brace for 6 weeks.
Range of motion: Early motion starts right away.
Ice and elevation: Used frequently to control pain and swelling. You should ice for 20 minutes 3-4 times a day right after surgery. An ice/compression machine can be hired from a 3rd party.
How Is the Wound Managed?
It is normal for the top dressing to become moist with arthroscopic fluid in the first 1–2 days.
After 1-2 days, remove the outer dressing and leave the smaller waterproof dressings in place.
Dressings may be removed completely after 7 days.
Incisions typically heal within two weeks.
Showers are permitted while the wounds are covered with waterproof dressings during the first 2 weeks.
Do not submerge incisions in water (baths, pools, ocean) for 4 weeks.
A wound check with your GP at the two-week mark is recommended.
Absorbable sutures are typically used and do not require removal, though occasionally small remnants may naturally surface during healing.
How Do I Prevent Blood Clots (DVT/PE)?
Blood clots (deep vein thrombosis or pulmonary embolism) are uncommon but can occur after surgery.
You can reduce the risk by:
Moving your foot and ankle regularly while resting.
Walking early with assistance.
You will likely be instructed to take aspirin for 2-4 weeks to prevent DVT/PE.
Avoiding long periods of sitting or immobility.
Seek immediate medical attention if you develop calf pain, swelling, chest pain, or shortness of breath.
How Do I Manage My Pain After PLC Reconstruction?
Use ice regularly (20 minutes at a time, several times per day). You may hire an ice machine from a 3rd party.
Take prescribed pain relief medications as directed. Opioid medication can be used, but there are known side effects such as nausea, vomiting, constipation, and dependence; thus, non-opioid medications should be prioritized when medically tolerated.
Use a compressive dressing on the knee for 6-12 weeks to help with swelling
Begin gentle range-of-motion and muscle activation exercises as soon as recommended.
Use walking aids to help with gait
What Issues Should I Call the Clinic Regarding?
You should contact your surgeon or clinic immediately if you notice:
Increasing redness, swelling, or foul-smelling drainage from the wound.
Persistent or worsening pain not controlled by medication.
Fever, chills, or night sweats.
Calf pain or swelling (possible blood clot).
Acute injury to your operative extremity.
Prompt review allows early management of potential complications.
When Can I Return to Normal Activities or Sports After PLC Reconstruction?
Because the PLC reconstruction is commonly performed with other knee ligament procedures, recovery is tailored to help the entire knee recover.
Return to activities depends on the nature and intensity of the recreation
This is a general guideline:
Running: once knee swelling, pain have resolved, and adequate strength has been retained- typically 4-5 months
Non-cutting activities/sport (golf, cricket, surfing, etc), typically 7-9 months
Training for sport, typically 9-12 months
Cutting sports (football, rugby, basketball, netball, etc), typically 12-18 months
There are no strict guidelines on when to return to sport after revision PCL reconstruction, but it typically takes 12-18 months.
When Can I Drive?
You can usually drive when you can safely control the vehicle and perform an emergency stop comfortably.
This is typically around 4–6 weeks after surgery for right knee surgery, and 2-3 weeks for the left knee.
You must not drive while taking strong pain medication (e.g., opioids).
When Can I Return to Work?
Return to work depends on your occupation:
Office or sedentary work: 1–2 weeks (once you can safely commute).
Light manual work: 4–6 weeks.
Heavy manual labour: 3–4 months or longer, depending on recovery.
Should I See a Physiotherapist?
Yes. Physiotherapy is essential for optimal recovery and long-term success after PLC reconstruction. Your physiotherapist will:
Guide you through a structured rehabilitation program.
Focus on restoring range of motion, strength, balance, and neuromuscular control.
Progress exercises gradually from early mobility to return-to-sport conditioning.
Most patients continue physiotherapy for 6–9 months to achieve full recovery, including returning to sport.
What Are the Complications After a PLC Reconstruction?
PLC reconstruction is a technically demanding procedure, but outcomes are excellent when performed correctly and followed by structured rehabilitation.
Potential complications include:
Infection (rare)
Wound healing complications
Blood clots (DVT/PE)
Knee stiffness or limited range of motion
Residual instability (especially with combined injuries)
Graft stretching or failure
Numbness or tingling around the incision
Injury to common peroneal nerve which can cause a disabling foot drop
Compartment Syndrome
Hardware irritation (may require removal)
Persistent swelling or discomfort
Progression of knee arthritis
Fracture
Donor site pain if the patients own tendon graft is harvested