
Abductor Tendon Repair
Anatomy of the Abductor Tendons
The hip abductor muscles — primarily the gluteus medius and gluteus minimus — are located on the outer side of the hip. These muscles originate from the outer surface of the pelvis and attach to the greater trochanter (the bony prominence on the upper part of the femur).
Their main function is to stabilize the pelvis during walking and to lift the leg to the side (abduction). Healthy abductor tendons are essential for walking without a limp, climbing stairs, and maintaining hip strength and balance.
Who Should Get an Abductor Tendon Repair?
Abductor tendon tears can occur from degenerative wear, chronic irritation, or trauma.
These injuries are often compared to a “rotator cuff tear of the hip.”
Surgery may be recommended if you have:
Persistent lateral hip pain that has not improved with physiotherapy, rest, or injections
MRI-confirmed partial or complete tendon tears
Loss of function (ie unable to manage stairs) or ongoing limp despite non-operative treatment
How Is the Abductor Tendon Repaired?
Abductor tendon repair is usually performed under general anaesthesia.
The procedure can be done endoscopically (keyhole) or through a mini-open incision, depending on tear size and tissue quality.
During surgery:
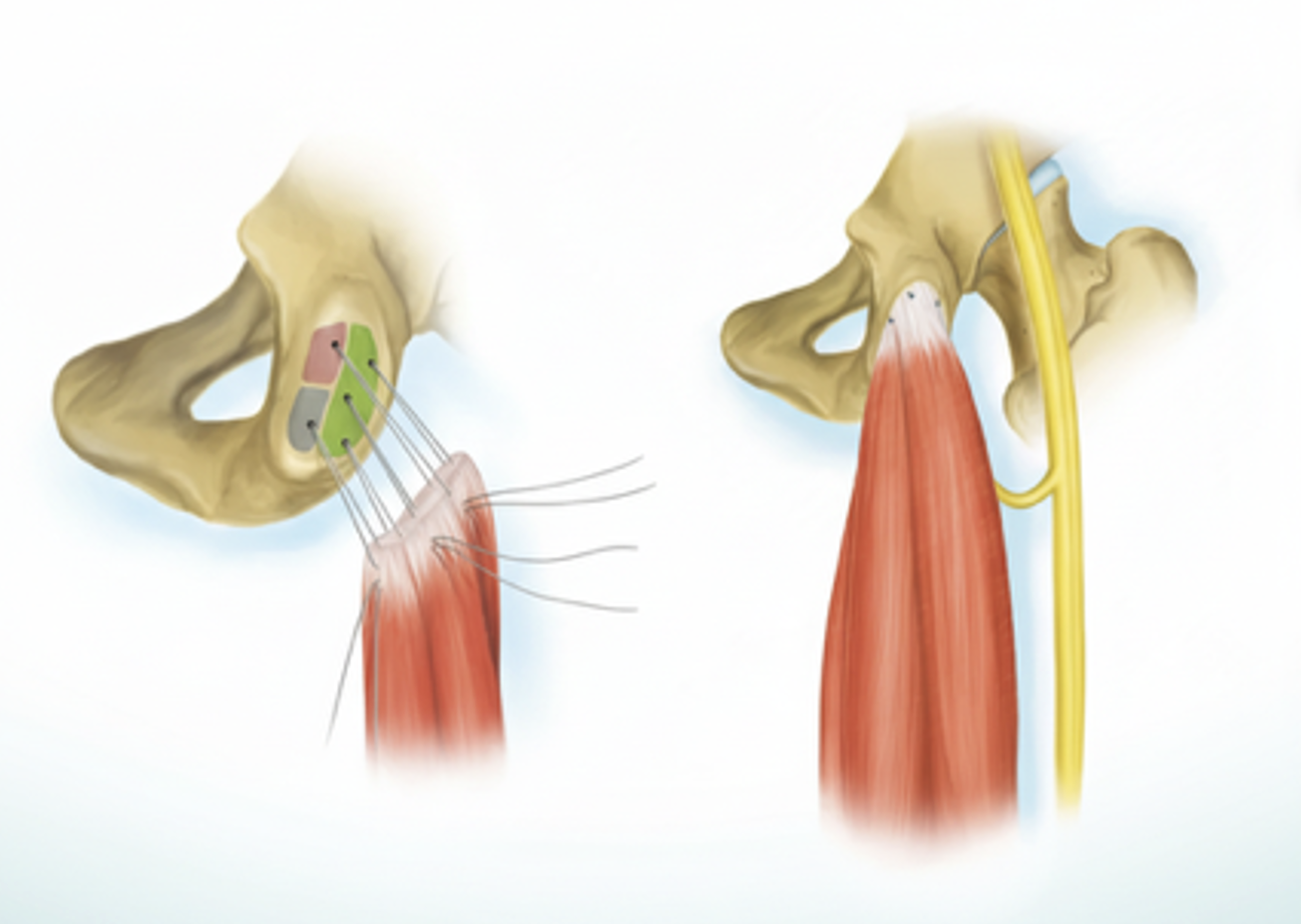
1. The torn edges of the gluteus medius and/or minimus tendons are identified.
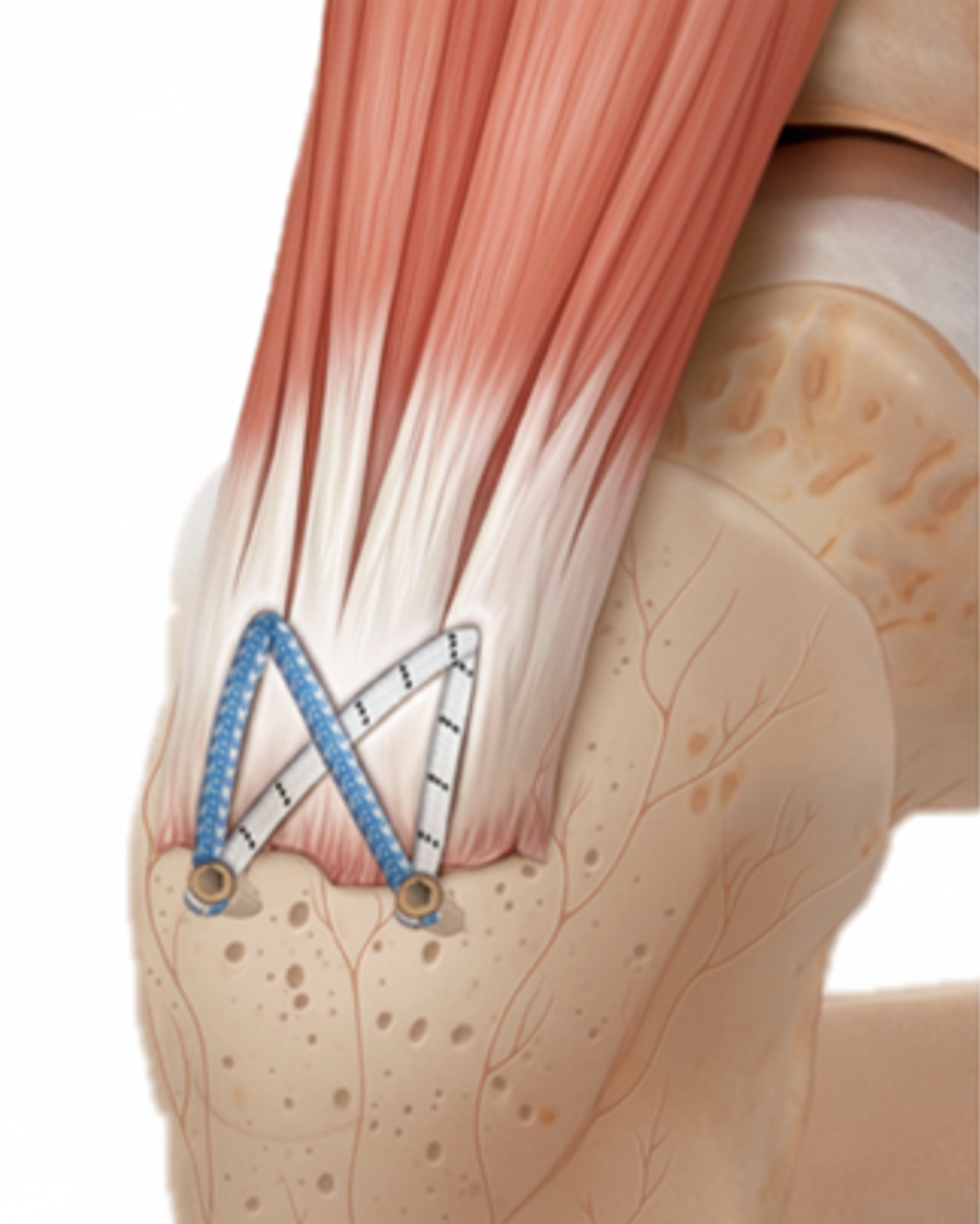
2. The surface of the greater trochanter is prepared to promote healing.
3. The tendons are securely reattached to the bone using strong suture anchors.
4. In chronic or large tears, a graft or augmentation may be used to reinforce the repair.
This restores the normal attachment of the abductor tendons, helping relieve pain and improve strength.
There are situations that the tendon cannot be repaired and a tendon transfer from gluteus maximus has to occur to improve the patient’s gait and pain.
How to Manage My Wound
Dressings: Your wound will be covered with a sterile dressing. Keep it clean and dry for the first 48 hours.
Showering: You may shower once the dressing is waterproof or as advised by your surgeon. Avoid soaking in baths or pools until the incision has fully healed.
Inspection: Check the wound daily for redness, swelling, drainage, or tenderness.
Sutures: Stitches or clips are generally removed at 10–14 days, unless dissolvable sutures are used.
Clothing: Avoid tight garments or pressure over the incision area.
If you notice increasing pain, discharge, fever, or spreading redness, contact your surgeon immediately.
What Is the Recovery for an Abductor Tendon Repair?
Rehabilitation is gradual and structured to protect the repair while restoring motion and strength:
Weeks 0–6: You will typically use crutches with partial weight bearing. No brace are typically required.
Weeks 6–12: Gradual increase in walking distance, gait training, and controlled strengthening exercises under physiotherapy guidance.
Months 3–6: Continued strengthening, balance work, and low-impact activity.
After 6 months: Return to higher-level activities as tolerated.
Most patients experience significant improvement in pain and function by 3–6 months.
When Can I Return to Activities?
Walking: Partial weight bearing immediately after surgery, progressing to full weight bearing by 6 weeks.
Low-impact exercise (bike, pool): Stationary bike can start right after surgery. Pool rehabilitation can start at 4 weeks.
Strength and balance training: Begins at 6–12 weeks.
Higher-impact activities (running): Usually at 6 months, depending on strength recovery and physiotherapist assessment.
When Can I Return to Work?
Sedentary/desk work: Usually 2–3 weeks after surgery if comfortable.
Light manual work: Around 4–8 weeks.
Heavy labour or physical jobs: May require 3–6 months, depending on recovery progress.
When Can I Return to Driving?
You may return to driving when you can comfortably sit and safely perform an emergency stop without pain or hesitation.
For an automatic transmission passage vehicle, typically returning to driving takes 2-3 weeks for the left leg and 8-10 weeks for the right leg.
What Complications Occur?
Abductor tendon repair is a safe operation, but as with any surgery, complications may occur. These include:
Wound issues: Infection, delayed healing, or sensitivity at the incision site.
Re-tear or incomplete healing: Particularly in large tears with poorly functioning muscle.
Persistent weakness or limp: May occur if tendon/muscle quality is poor or rehabilitation is incomplete. Some patients may still require lifelong use of walking assistance.
Deep vein thrombosis/Pulmonary Embolism: Preventative measures are used to minimize this risk via blood thinners such as aspirin.
Fracture: Very rare, more common in patients with poor bone quality.